
Get started with SKYCLARYS.
Biogen REACH is here for your
eligible patients
Quick highlights1
- SKYCLARYS is a once-daily oral prescription medicine
- Some inhibitors and even foods like grapefruit can interfere with treatment. See more details below
- Increases in ALT/AST were generally asymptomatic and reversible. Maximum increases in ALT and AST occurred within 12 weeks of starting SKYCLARYS

SKYCLARYS is a once-daily oral prescription medicine1
The recommended dose is 150 mg taken as 3 capsules (50 mg each) once daily.1
For patients taking SKYCLARYS1:
- Take on an empty stomach 1 hour before eating
- Swallow SKYCLARYS capsules whole. Do not crush or chew
- Avoid grapefruit and grapefruit juice
- If a dose of SKYCLARYS is missed, take the next dose at its scheduled time the following day. A double dose should not be taken to make up for a missed dose
- Discuss all medications they are taking, including other prescription medications, non-prescription medications, or herbal products (eg, St. John’s wort)
For patients who are unable to swallow whole capsules1:
- SKYCLARYS capsules may be opened and the entire contents of both halves of the capsule sprinkled onto 2 tablespoons (30 mL) of applesauce
- Stir the mixture until homogenous
- Swallow all the drug/applesauce mixture immediately
- Do not store the mixture for future use
- Contents of the SKYCLARYS capsules should not be mixed with milk or orange juice
- Not for enteral feeding tube administration
Additional dosing and administration considerations for patients taking SKYCLARYS1:
For additional information about SKYCLARYS dosing as it relates to concomitant use with strong or moderate CYP3A4 inhibitors/inducers, patients with hepatic impairment, and the use of hormonal contraceptives, please see the full Prescribing Information.
Consult the full Prescribing Information for specific dosing considerations for these patients.

Warnings and precautions1
Elevation of aminotransferases
Treatment with SKYCLARYS can cause an elevation in hepatic transaminases (ALT and AST).

Monitor ALT, AST, and total bilirubin prior to initiation of SKYCLARYS, every month for the first 3 months of treatment, and periodically thereafter.
If transaminases increase to levels greater than 5 times the ULN, or greater than 3 times the ULN with evidence of liver dysfunction (eg, elevated bilirubin), immediately discontinue SKYCLARYS and repeat liver function tests as soon as possible.
If transaminase levels stabilize or resolve, SKYCLARYS may be reinitiated with an appropriate increased frequency of monitoring of liver function.
Maximum increases in ALT and AST occurred within 12 weeks after starting SKYCLARYS. Increases in serum aminotransferases were generally asymptomatic and reversible following discontinuation of SKYCLARYS.
Elevation of B-type natriuretic peptide (BNP)
Treatment with SKYCLARYS can cause an increase in BNP, a marker of cardiac function. Elevations in BNP may indicate cardiac failure and should prompt an evaluation of cardiac function. Check BNP prior to initiation of SKYCLARYS.
Monitor patients for the signs and symptoms of fluid overload, such as sudden weight gain (3 pounds or more of weight gain in one day, or 5 pounds or more of weight gain in a week), peripheral edema, palpitations, and shortness of breath. Management of fluid overload and heart failure may require discontinuation of SKYCLARYS.
Lipid abnormalities
Treatment with SKYCLARYS can cause changes in cholesterol.
Mean increases were observed within 2 weeks of initiation of SKYCLARYS and returned to baseline within 4 weeks of discontinuing treatment. Assess lipid parameters prior to initiation of SKYCLARYS and monitor periodically during treatment.
ALT=alanine aminotransferase,
AST=aspartate aminotransferase,
ULN=upper limit of normal.
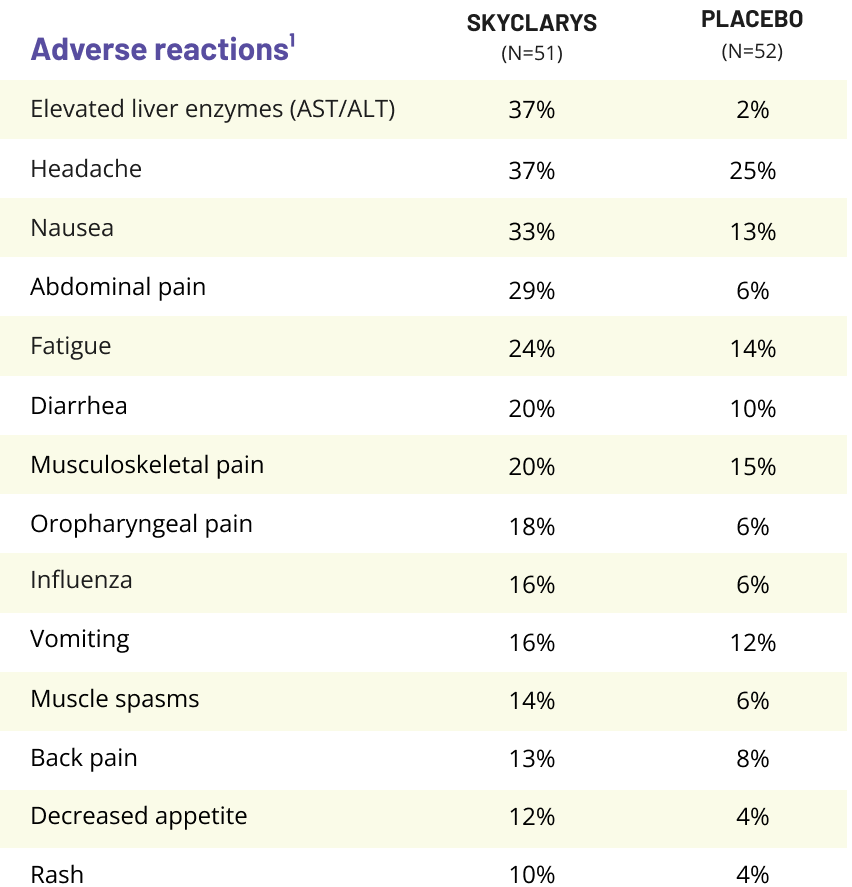
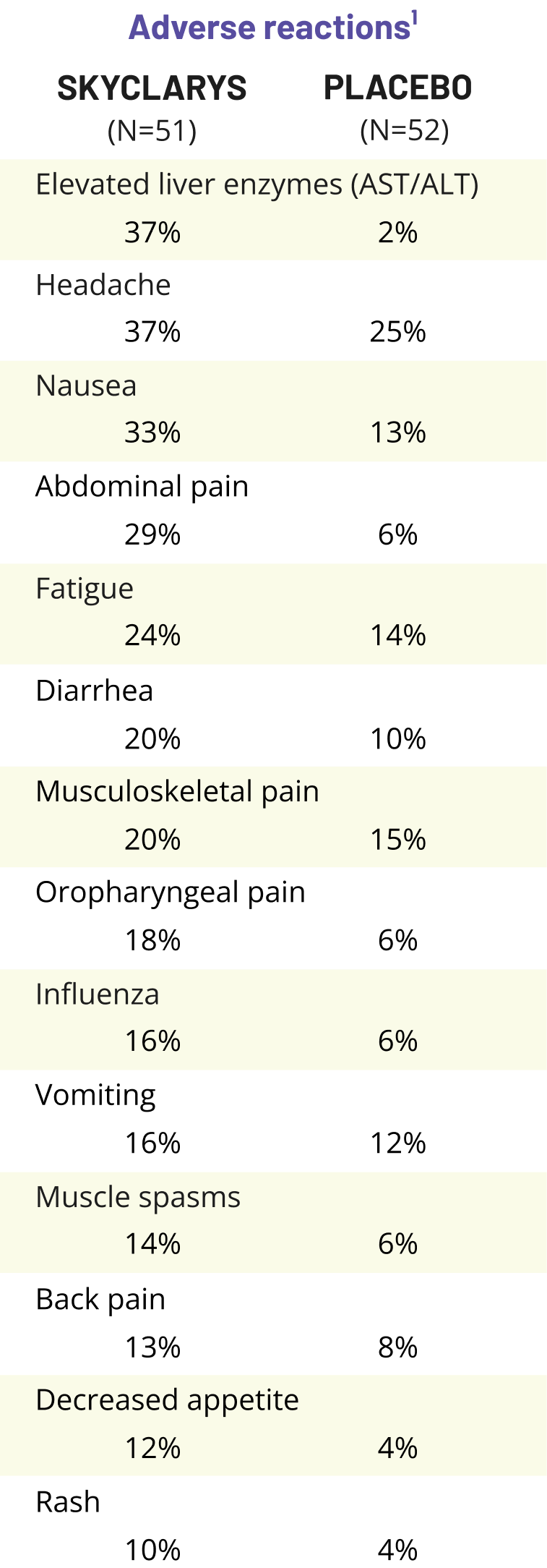
Safety data from the MOXIe trial1,2
Adverse events were generally considered mild to moderate.
The most common adverse reactions (≥20% and greater than placebo) were elevated liver enzymes (AST/ALT), headache, nausea, abdominal pain, fatigue, diarrhea, and musculoskeletal pain.1
Adverse reactions reported in ≥10% of patients and greater than placebo.
References:
1. Skyclarys. Prescribing Information. Biogen; 2024. 2. Lynch DR, Chin MP, Delatycki MB, et al. Safety and efficacy of omaveloxolone in Friedreich ataxia (MOXIe study). Ann Neurol. 2021;89(2):212-225. doi:10.1002/ana.25934 3. Parkinson MH, Boesch S, Nachbauer W, Mariotti C, Giunti P. Clinical features of Friedreich’s ataxia: classical and atypical phenotypes. J Neurochem. 2013;126(suppl 1):103-117. doi:10.1111/jnc.12317 4. Schulz JB, Boesch S, Bürk K, et al. Diagnosis and treatment of Friedreich ataxia: a European perspective. Nat Rev Neurol. 2009;5(4):222-234. doi:10.1038/nrneurol.2009.26 5. Rummey C, Farmer JM, Lynch DR. Predictors of loss of ambulation in Friedreich’s ataxia. eClinicalMedicine. 2020;18:1-9. doi:10.1016/j.eclinm.2019.11.006 6. Rummey C, Corben LA, Delatycki MB, et al. Psychometric properties of the Friedreich Ataxia Rating Scale. Neurol Genet. 2019;5(6):371. doi:10.1212/NXG.0000000000000371 7. Patel M, Isaacs CJ, Seyer L, et al. Progression of Friedreich ataxia: quantitative characterization over 5 years. Ann Clin Transl Neurol. 2016;3(9):684-694. doi:10.1002/acn3.332 8. Lynch DR, Chin MP, Boesch S, et al. Efficacy of omaveloxolone in Friedreich’s ataxia: delayed-start analysis of the MOXIe extension. Mov Disord. 2023;38(2):313-320. doi:10.1002/mds.29286 9. Galea CA, Huq A, Lockhart PJ, et al. Compound heterozygous FXN mutations and clinical outcome in Friedreich ataxia. Ann Neurol. 2016;79(3):485-495. doi:10.1002/ana.24595 10. Fogel BL, Perlman S. Clinical features and molecular genetics of autosomal recessive cerebellar ataxias. Lancet Neurol. 2007;6(3):245-257. 11. Wallace SE, Bird TD. Molecular genetic testing for hereditary ataxia: what every neurologist should know. Neurol Clin Pract. 2018;8(1):27-32. doi:10.1212/CPJ.0000000000000421 12. Data on file. Reata Pharmaceuticals, Inc.; 2022. 13. Lynch DR, Goldsberry A, Rummey C, et al. Propensity matched comparison of omaveloxolone treatment to Friedreich ataxia natural history data. Ann Clin Transl Neurol. 2024;11(1):4-16. doi:10.1002/acn3.51897
14. Beaulieu-Jones BK, Finlayson SG, Yuan W, et al. Examining the use of real-world evidence in the regulatory process. Clin Pharmacol Ther. 2020;107(4):843-852. doi:10.1002/cpt.1658